Is It Perimenopause? Ten Early Signs that Women May Not Recognize
Something Feels Off
Maybe it started with sleep that just isn't as deep as it used to be, or a wave of anxiety that appeared out of nowhere. Maybe your periods shifted, just slightly, or you've noticed a stubborn few pounds around your midsection that won't budge no matter what you do. You've chalked it up to stress, to aging, to being busy. But what if there's a deeper explanation?
For many women, perimenopause begins years before menopause itself: sometimes in the late 30s or early 40s. And the earliest symptoms are often the ones that get overlooked. Periods may still be regular. Lab work may come back "normal." And because the hallmark symptoms like hot flashes haven't arrived yet, the connection to hormones is easy to miss.
Here's what's important to understand: perimenopause isn't driven by low hormones alone. It's driven by fluctuating hormones: unpredictable rises and falls in estrogen and progesterone that can create a wide range of symptoms long before your period ever stops. Research shows that greater estradiol variability and declining progesterone are independently associated with mood and sleep disruption during this transition, even when hormone levels appear to be in the "normal" range on a single blood draw [4].
If you've been feeling unlike yourself and can't quite pinpoint why, this article is for you.
What Is Perimenopause?
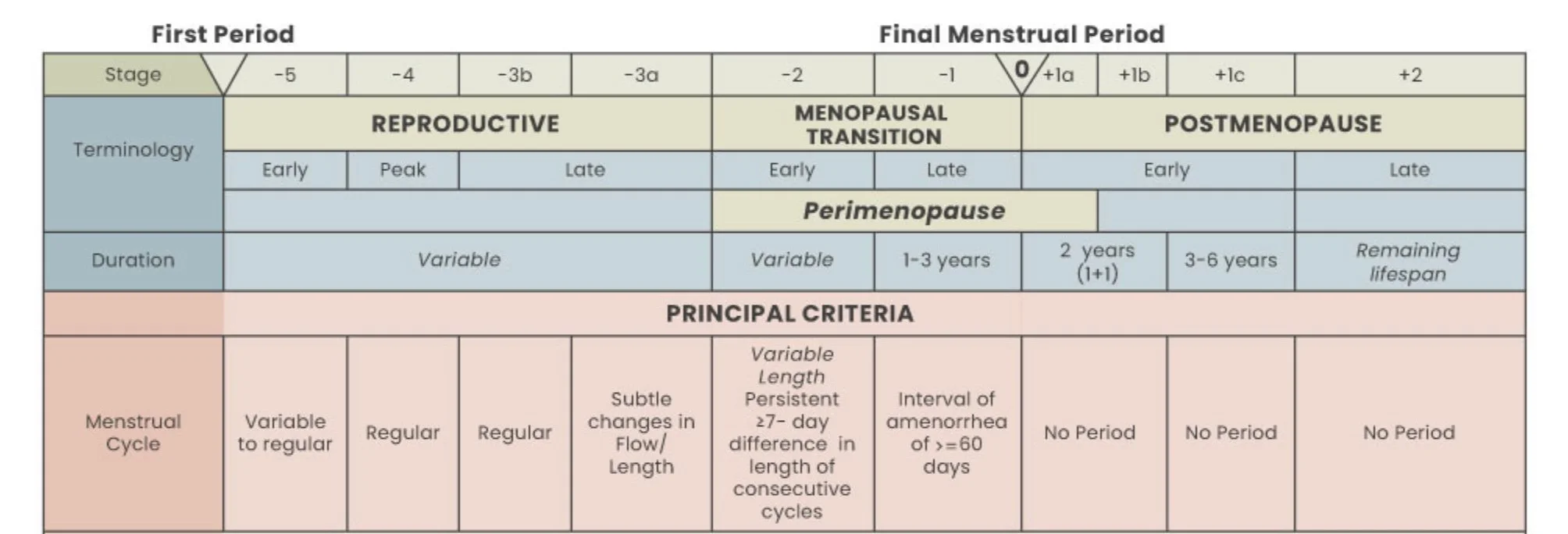
Perimenopause is the transitional phase leading up to menopause: the point when menstruation permanently stops. While menopause itself is defined as 12 consecutive months without a period, perimenopause is the stretch of time before that final period, when ovarian function gradually shifts and hormone levels become increasingly variable.
The menopausal transition is divided into two stages. The early transition begins when menstrual cycle length starts to vary: a persistent difference of seven or more days between consecutive cycles. The late transition is marked by stretches of amenorrhea lasting 60 days or longer. Perimenopause encompasses both of these stages plus the first 12 months after the final menstrual period [2].
Stages of Perimenopause and Menopause
What makes perimenopause so confusing is the nature of the hormonal changes. Estradiol levels don't simply decline in a straight line — they fluctuate wildly, sometimes spiking higher than premenopausal levels before dropping. Progesterone declines as ovulation becomes less consistent. Follicle-stimulating hormone (FSH) rises but can swing back to premenopausal levels from one cycle to the next. This hormonal variability is what drives the unpredictable, seemingly random nature of perimenopausal symptoms [4].
Understanding this is key: it's not just about hormones being low. It's about hormones being unstable.
At What Age Does Perimenopause Start?
The average age of menopause in North America is approximately 51 years, and perimenopause typically begins four to eight years before that, meaning many women enter this transition in their mid-40s, with the median age of onset around 47 years. However, there is significant variability. Some women begin experiencing perimenopausal symptoms in their early 40’s, or even late 30s [3].
Several factors can influence timing:
Family history: The age at which your mother or sisters experienced menopause can be a rough predictor of your own timeline.
Smoking: Cigarette smokers tend to undergo menopause approximately two years earlier than nonsmokers [1].
Surgical history: Women who have had a hysterectomy (even with ovaries preserved) or ovarian surgery may experience an earlier transition.
Primary ovarian insufficiency: In some women, ovarian function declines before age 40, which is considered premature.
The duration of perimenopause also varies widely. Studies have reported mean durations ranging from approximately 4 to 8 years, though the menopause transition can last over a decade for some women [3].
The key takeaway: if you're in your late 30s or early 40s and experiencing symptoms that feel new or unexplained, perimenopause is worth considering; even if it feels "too early."
Ten Early Signs of Perimenopause
1. Changes in Your Menstrual Cycle
One of the earliest and most reliable signs of perimenopause is a shift in your menstrual cycle. And it doesn't always look the way you'd expect.
What it feels like: Your cycle may get shorter before it gets longer. Periods that were once predictably 28 days may start arriving every 24 or 25 days. Some months, bleeding may be noticeably heavier. Later, you may begin skipping periods altogether.
Why it happens: As ovarian reserve declines, the follicular phase of the menstrual cycle shortens, leading to shorter overall cycle length. Fluctuating estrogen levels can cause the uterine lining to build up more than usual, resulting in heavier or prolonged bleeding. Irregular ovulation means progesterone, which normally stabilizes the lining, may be absent or insufficient in some cycles [2].
Why women often miss it: A cycle that shifts from 28 to 25 days still feels "regular." Many women don't track their cycles closely enough to notice a gradual change, and heavier periods may be attributed to fibroids or stress rather than hormonal shifts.
When to seek evaluation: If you're experiencing cycles shorter than 21 days, bleeding that lasts longer than seven days, or bleeding heavy enough to soak through a pad or tampon every hour, it's worth discussing with a clinician, both to evaluate for perimenopause and to rule out other causes [1].
2. Sleep Problems or Waking Up at 3 AM
If you've started waking in the middle of the night alert, restless, sometimes drenched in sweat, you're not alone. Sleep disturbance affects between 40% and 69% of women during the menopausal transition, with up to 40% meeting diagnostic criteria for insomnia disorder [6].
What it feels like: Difficulty falling asleep, frequent nighttime awakenings, or waking at 3 or 4 AM and being unable to fall back asleep. Some women notice night sweats; others simply feel wired or restless.
Why it happens: The decline in estrogen and progesterone directly affects sleep architecture. Progesterone has natural sedative properties, and its decline during perimenopause can contribute to lighter, more fragmented sleep. Research has shown that lower estradiol and higher FSH levels are associated with more frequent nighttime awakenings, independent of night sweats or mood symptoms [7]. Vasomotor symptoms (night sweats) compound the problem, and women with moderate to severe vasomotor symptoms are nearly three times as likely to report frequent nocturnal awakenings. Additionally, heightened stress reactivity from declining hormone levels can increase pre-sleep arousal and negative cognitions about sleep [6].
Why women often miss it: Sleep disruption is so common in busy, stressed adults that it's easy to blame lifestyle factors. Without obvious night sweats, the hormonal connection may not be apparent.
When to seek evaluation: Persistent sleep disruption that affects daytime functioning, mood, or cognitive performance warrants a conversation with a provider, especially if it's a new pattern that began in your late 30s or 40s.
3. Anxiety, Panic Attacks, or Feeling "On Edge"
Perhaps one of the most unsettling early symptoms of perimenopause is the sudden onset of anxiety, especially in women who have never experienced it before.
What it feels like: A sense of dread or unease that seems to come from nowhere. Heart racing. Feeling overwhelmed by things that used to feel manageable. Some women experience full panic attacks for the first time in their lives.
Why it happens: Estrogen plays a significant role in regulating neurotransmitters in the brain, including serotonin, dopamine, and GABA (gamma-aminobutyric acid). When estrogen levels fluctuate unpredictably during perimenopause, these neurotransmitter systems become destabilized, which can trigger anxiety, irritability, and emotional reactivity. Research has demonstrated that women in perimenopause have an increased risk of developing mood disorders, including anxiety and depression, regardless of whether they have a prior psychiatric history [5]. Greater estradiol variability and the absence of ovulatory progesterone levels have been independently associated with higher levels of depressive and anxious symptoms [4].
Why women often miss it: New-onset anxiety in midlife is frequently attributed to life stress: work, parenting, aging parents, relationship strain. Without recognizing the hormonal connection, women may spend months or years seeking treatment for anxiety alone without addressing the underlying hormonal shifts.
When to seek evaluation: If you're experiencing new or worsening anxiety, especially alongside other symptoms on this list, a comprehensive evaluation that includes a discussion of your menstrual and hormonal history can help clarify whether perimenopause may be a contributing factor.
4. Brain Fog and Difficulty Concentrating
Forgetting why you walked into a room. Struggling to find the right word. Losing your train of thought mid-sentence. These cognitive shifts are among the most commonly reported, and most distressing symptoms of perimenopause.
What it feels like: Difficulty concentrating, memory lapses, trouble with word retrieval, and a general sense that your thinking is "slower" or less sharp. Women who have ADHD may notice a significant worsening of symptoms. Executive function: the ability to plan, organize, and multitask, can feel noticeably impaired.
Why it happens: Estradiol is a master regulator of metabolic function in the brain, influencing glucose metabolism, neuronal connectivity, and neurotransmitter activity. During perimenopause, the volatile withdrawal of estradiol can lead to widespread changes in brain structure, connectivity, and energy metabolism, essentially creating a temporary hypo-metabolic state. A 2026 meta-analysis of 26 studies found that perimenopausal women exhibited poorer cognitive outcomes than premenopausal women, with a moderate effect size [8]. Importantly, research also suggests that many of these cognitive changes stabilize or even revert after the transition to postmenopause, indicating a compensatory mechanism in the brain [8].
Why women often miss it: Brain fog is easily attributed to stress, poor sleep, or simply "getting older." Many women worry they're developing dementia, when in reality, the cognitive changes of perimenopause, while real and measurable, typically remain within normal functional limits.
When to seek evaluation: If cognitive changes are affecting your work performance, daily functioning, or causing significant distress, it's worth discussing with a provider. Ruling out other causes (thyroid dysfunction, sleep disorders, depression) is important, and understanding the hormonal context can provide reassurance and guide management.
5. Weight Gain Around the Midsection
You haven't changed your diet. You haven't stopped exercising. And yet, your body is changing — particularly around your waist.
What it feels like: A gradual increase in abdominal fat that feels resistant to the strategies that used to work. Clothes fitting differently. A shift in body composition even if the number on the scale hasn't changed dramatically.
Why it happens: The menopausal transition is associated with significant changes in body composition and fat distribution. Declining estrogen promotes a shift from subcutaneous (under-the-skin) fat storage to visceral (abdominal) fat accumulation. This shift is metabolically significant: visceral fat is associated with increased insulin resistance, changes in lipid profiles, and elevated cardiovascular risk [2]. Simultaneously, loss of lean muscle mass accelerates during this period, which lowers resting metabolic rate and makes weight management more challenging [1].
Why women often miss it: Weight gain in midlife is often attributed to aging, lifestyle, or stress. The specific pattern of central fat accumulation, and its hormonal driver, is frequently overlooked.
When to seek evaluation: If you're noticing unexplained changes in body composition, especially alongside other perimenopausal symptoms, a metabolic and hormonal evaluation can help identify contributing factors and guide a personalized approach to nutrition, exercise, and hormonal support (when appropriate).
Learn more about weight gain in perimenopause
6. Fatigue and Loss of Energy
This isn't the tiredness that comes from a late night. It's a bone-deep exhaustion that doesn't fully resolve with rest.
What it feels like: Persistent low energy. Feeling drained by mid-afternoon. Needing more recovery time after physical or mental exertion. A sense that your "battery" doesn't charge the way it used to.
Why it happens: Perimenopausal fatigue is multifactorial. Disrupted sleep (whether from night sweats, insomnia, or hormonal effects on sleep architecture) is a major contributor [6]. But fatigue can also result directly from hormonal fluctuations affecting the central nervous system, changes in muscle mass and physical function, and the cumulative burden of other perimenopausal symptoms like mood disruption and cognitive strain [5]. A large analysis of over 145,000 symptom logs found that fatigue was one of the most commonly reported symptoms across all stages of the menopausal transition (premenopause, perimenopause, and postmenopause alike) highlighting how pervasive and persistent this symptom can be [1].
Why women often miss it: Fatigue is universal. Everyone is tired. It's easy to normalize, and it rarely prompts a visit to the doctor on its own.
When to seek evaluation: When fatigue is persistent, disproportionate to your activity level, and accompanied by other symptoms on this list, it's worth exploring the hormonal connection. Thyroid function, iron levels, and sleep quality should also be assessed.
7. Mood Changes or Increased Irritability
This is different from anxiety. This is the feeling of being emotionally raw: quick to anger, quick to tears, quick to feel overwhelmed by things that wouldn't have fazed you before.
What it feels like: Emotional volatility. Disproportionate irritability (sometimes described as "rage") over minor frustrations. Low frustration tolerance. Feeling emotionally sensitive or reactive in ways that feel unfamiliar.
Why it happens: Estrogen and progesterone fluctuations during perimenopause have a profound effect on the central nervous system, creating an imbalance between excitatory and inhibitory neural inputs. Changes in serotonin, dopamine, GABA, and neurosteroids like allopregnanolone all contribute to mood instability [5]. The menopausal transition is associated with higher rates of major depression, with approximately 10% of perimenopausal and postmenopausal women experiencing an episode of major depression. Women with a history of depression are at particularly elevated risk [5].
Why women often miss it: Mood changes are often attributed to life circumstances. The hormonal contribution is frequently unrecognized, especially when a woman is still having regular periods.
When to seek evaluation: If mood changes are affecting your relationships, work, or quality of life, or if you're experiencing symptoms of depression, a provider who understands the hormonal landscape of perimenopause can help distinguish between situational mood changes and those driven by the menopausal transition.
8. Joint Pain, Frozen Shoulder, or Body Aches
This is one of the most under-recognized symptoms of perimenopause, and one of the most common. More than 70% of women experience musculoskeletal symptoms during the transition from perimenopause to postmenopause, and 25% will be significantly disabled by them [9].
What it feels like: Stiffness in the morning. Aching joints, especially in the hands, knees, and shoulders. New onset of tendon pain or frozen shoulder. A general sense that your body feels older than it should.
Why it happens: Estrogen plays a critical role in maintaining the health of joints, tendons, cartilage, and connective tissue. It has anti-inflammatory, antifibrotic, and antioxidant properties that protect musculoskeletal structures. As estrogen levels decline and fluctuate during perimenopause, these protective effects diminish [10]. Joint pain and stiffness are significantly more common in postmenopausal women than in premenopausal women, independent of chronological age [9]. Frozen shoulder, in particular, has been increasingly recognized as linked to estrogen deficiency during perimenopause, with research demonstrating that estrogen depletion contributes to capsular fibrosis through specific molecular pathways. Researchers have recently proposed the term "musculoskeletal syndrome of menopause" to describe this constellation of symptoms [9].
Why women often miss it: Joint pain in midlife is typically attributed to aging, overuse, or early arthritis. The connection to hormonal changes is rarely made by women or their clinicians.
When to seek evaluation: If you're experiencing new or worsening joint pain, stiffness, or tendon problems, especially alongside other perimenopausal symptoms, it's worth considering the hormonal contribution as part of your evaluation.
9. Hot Flashes or Night Sweats
Many women believe hot flashes only happen around the time of menopause itself. In reality, vasomotor symptoms can begin during perimenopause (sometimes years before the final period) and may initially be subtle or intermittent.
What it feels like: A sudden wave of heat, often starting in the chest or face, sometimes accompanied by flushing, sweating, and a rapid heartbeat. Night sweats may drench your sheets. Episodes can last from seconds to several minutes and may occur multiple times a day, or only occasionally.
Why it happens: Vasomotor symptoms result from changes in the brain's thermoregulatory center, driven by fluctuating estrogen levels and shifts in neurotransmitter signaling, particularly involving kisspeptin and neurokinin B pathways. Up to 80% of women experience vasomotor symptoms during the menopausal transition. Longitudinal data show that moderate to severe vasomotor symptoms last a median of 7.4 years [1].
Why women often miss it: Early vasomotor symptoms may be mild, infrequent, or mistaken for feeling overheated due to exercise, stress, or warm environments. Women who experience night sweats without daytime hot flashes may not connect the dots.
When to seek evaluation: Any new-onset vasomotor symptoms (even mild ones) are worth mentioning to your provider, as they can be an early indicator of the menopausal transition and may benefit from treatment.
10. Low Libido or Vaginal Dryness
Changes in sexual desire and comfort are among the most common, and most under-treated, symptoms of the menopausal transition.
What it feels like: A noticeable decline in sexual interest or arousal. Vaginal dryness, burning, or irritation. Pain or discomfort during intercourse. A sense that your body's sexual response has fundamentally changed.
Why it happens: Declining estrogen leads to structural changes in the vaginal wall, including thinning of the epithelium, reduced blood flow, and decreased lubrication: a constellation of symptoms now known as genitourinary syndrome of menopause (GSM). GSM affects an estimated 45% to 77% of women and, unlike vasomotor symptoms, tends to worsen over time without treatment [1]. Changes in testosterone levels may also contribute to decreased sexual desire. Sexual dysfunction increases from approximately 27% in women aged 18 to 44 to nearly 45% in women aged 45 to 64 [5].
Why women often miss it: Many women feel embarrassed to bring up sexual concerns, or they assume these changes are simply a natural part of aging that must be accepted. In reality, effective treatments exist.
When to seek evaluation: If vaginal dryness, pain with intercourse, or changes in sexual desire are affecting your quality of life or your relationship, these symptoms deserve attention. A range of treatment options, from vaginal moisturizers to local estrogen therapy to systemic hormonal approaches, can make a meaningful difference.
Why Perimenopause Is Often Missed
If you've read through this list and thought, "That's me, but no one has ever mentioned perimenopause," you're not alone. There are several reasons this transition is so frequently overlooked:
Symptoms are attributed to stress or aging. Fatigue, anxiety, sleep disruption, weight gain, brain fog: every one of these symptoms has a dozen other plausible explanations. Without a clinician who thinks to ask about menstrual patterns and hormonal history, the connection to perimenopause may never be made.
Lab work may appear "normal." Hormone levels during perimenopause are inherently variable. FSH and estradiol can swing between premenopausal and postmenopausal ranges from one week to the next. A single blood draw captures only a snapshot and may be misleading. As highlighted by the ABIM Foundation's Choosing Wisely campaign, measuring FSH in women in their 40s is not recommended for identifying the menopausal transition, because these values fluctuate too much to be diagnostically useful [3].
Women may still be having regular periods. Perimenopause can begin while cycles are still relatively regular, especially in the early transition, when the primary change may be a subtle shortening of cycle length rather than missed periods [2].
Fluctuating hormones create confusing symptom patterns. Symptoms may come and go unpredictably. A woman might have a terrible month of insomnia and anxiety, followed by a month where she feels fine. This inconsistency makes it hard to identify a pattern [4].
Many clinicians receive limited menopause training. A survey of U.S. residency programs found that only 6.8% of residents in family medicine, internal medicine, and obstetrics and gynecology felt adequately prepared to manage women experiencing menopause. Over 20% reported receiving no menopause lectures during their entire residency [11]. A more recent survey found that the most frequently reported barrier to providing menopause care was lack of training, cited by 62% of providers [12].
This is not a reflection of any individual clinician's competence; it's a systemic gap in medical education that is only now beginning to be addressed.
How Is Perimenopause Diagnosed?
Perimenopause is primarily a clinical diagnosis: meaning it's based on your symptoms, your age, and your menstrual history, not on a single lab test [3].
The diagnosis of the menopausal transition (aka perimenopause) is made based on age, menstrual irregularity, and the presence of characteristic symptoms. A thorough clinical history (including changes in cycle length, bleeding patterns, sleep, mood, cognitive function, and other symptoms) is the most valuable diagnostic tool [1].
The limitations of hormone testing are important to understand. FSH and estradiol levels fluctuate dramatically during perimenopause: varying from cycle to cycle, week to week, and even within a single day. These values do not stabilize at postmenopausal levels until three to six years after the final menstrual period. For this reason, routine measurement of FSH or estradiol is not recommended for diagnosing perimenopause in women in their 40s [3]. Hormone testing may be appropriate in specific situations (such as evaluating for premature ovarian insufficiency in women under 40, or assessing fertility) but it is not a reliable way to confirm or rule out perimenopause.
What matters most is finding a clinician who will listen to your full story, recognize the patterns, and provide an individualized evaluation. Perimenopause doesn't look the same in every woman, and a one-size-fits-all approach (whether to diagnosis or treatment) misses the mark.
You Don't Have to "Just Push Through"
If anything in this article resonated with you, know this: what you're experiencing is real, it's common, and it's not something you simply have to endure.
Perimenopause is a significant biological transition: one that affects the brain, the body, sleep, mood, metabolism, and quality of life. The symptoms are not "in your head," and they're not a sign of weakness. They are the predictable result of a major shift in your hormonal landscape [5].
The good news is that effective, evidence-based options exist: from lifestyle strategies to hormonal and non-hormonal therapies. And the right approach depends on your individual symptoms, health history, and goals. The first step is recognition. The second is finding a provider who takes these symptoms seriously and has the training to help [11, 12]. One reputable credential that may help identify clinicians with additional menopause-specific training is Menopause Society Certified Practitioner (MSCP).
You deserve to feel like yourself again. Book a free discovery call to learn more.
Frequently Asked Questions
Can you be in perimenopause with regular periods?
Yes. Perimenopause can begin while periods are still relatively regular. The earliest changes may involve subtle shifts in cycle length (such as cycles becoming a few days shorter) before any periods are actually missed. Symptoms like sleep disruption, mood changes, and brain fog can appear well before menstrual irregularity becomes obvious [2].
What age does perimenopause usually start?
The median age of onset is approximately 47 years, but perimenopause can begin in the early-to-mid 40s for many women, and occasionally in the late 30s. By age 45, roughly 40% of women have already entered the menopausal transition [3].
How long does perimenopause last?
The duration varies widely. On average, perimenopause lasts approximately four to eight years, though some women experience a shorter or longer transition. The menopause transition can last over a decade in some cases [3].
Can perimenopause cause anxiety?
Yes. Fluctuating estrogen and progesterone levels during perimenopause affect neurotransmitter systems in the brain (including serotonin, dopamine, and GABA) which can trigger new-onset anxiety, even in women with no prior history of anxiety disorders [5].
Can perimenopause cause weight gain?
Yes. The hormonal shifts of perimenopause promote changes in body composition, including increased visceral (abdominal) fat, decreased lean muscle mass, and changes in insulin sensitivity and lipid metabolism. These changes can make weight management more challenging even without changes in diet or exercise [2].
What are the first signs of perimenopause?
The earliest signs often include changes in menstrual cycle length (typically shorter cycles), sleep disruption, new or worsening anxiety, brain fog, and fatigue. Hot flashes and missed periods may come later in the transition [1, 4].
Is 35 too early for perimenopause?
While uncommon, some women do begin experiencing perimenopausal symptoms in their mid-to-late 30s. If menopause occurs before age 40, it is classified as premature ovarian insufficiency and warrants specific evaluation and management. However, early perimenopausal symptoms in the late 30s, while less typical, are not unheard of and should be taken seriously [3].
Can hormone levels test normal during perimenopause?
Yes, and this is one of the most important things to understand. Hormone levels during perimenopause fluctuate dramatically, and a single blood draw may capture a moment when levels appear completely normal. This is why perimenopause is diagnosed based on clinical symptoms and history, not on a single lab result [3].
References
1. Crandall, C. J., Mehta, J. M., & Manson, J. E. (2023). Management of menopausal symptoms: A review. JAMA, 329(5), 405–420. https://pubmed.ncbi.nlm.nih.gov/36749328/
2. El Khoudary, S. R., Aggarwal, B., Beckie, T. M., et al. (2020). Menopause transition and cardiovascular disease risk: Implications for timing of early prevention: A scientific statement from the American Heart Association. Circulation, 142(25), e506–e532. https://pubmed.ncbi.nlm.nih.gov/33251828/
3. Bastian, L. A., Smith, C. M., & Nanda, K. (2003). Is this woman perimenopausal? JAMA, 289(7), 895–902. https://pubmed.ncbi.nlm.nih.gov/12588275/
4. Joffe, H., de Wit, A., Coborn, J., et al. (2020). Impact of estradiol variability and progesterone on mood in perimenopausal women with depressive symptoms. Journal of Clinical Endocrinology and Metabolism, 105(3), e642–e650. https://pubmed.ncbi.nlm.nih.gov/31693131/
5. Brown, L., Hunter, M. S., Chen, R., et al. (2024). Promoting good mental health over the menopause transition. Lancet, 403(10430), 969–983. https://pubmed.ncbi.nlm.nih.gov/38458216/
6. Breitinger-Blatt, D., Lee, J., Ribeiro Pereira, S. I., et al. (2026). Cognitive behavioural therapeutics for insomnia symptoms in the perimenopause through to the early postmenopausal period. Cochrane Database of Systematic Reviews.https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD016349/full
7. Coborn, J., de Wit, A., Crawford, S., et al. (2022). Disruption of sleep continuity during the perimenopause: Associations with female reproductive hormone profiles. Journal of Clinical Endocrinology and Metabolism, 107(7), e2813–e2822. https://pubmed.ncbi.nlm.nih.gov/35878624/
8. Bangle, A., Williams, D., Walters, J., & Nguyen, L. (2026). Cognitive functioning in perimenopause: An updated systematic review and meta-analysis. Psychology and Aging. https://pubmed.ncbi.nlm.nih.gov/41066270/
9. Wright, V. J., Schwartzman, J. D., Itinoche, R., & Wittstein, J. (2024). The musculoskeletal syndrome of menopause. Climacteric, 27(5), 466–472. https://pubmed.ncbi.nlm.nih.gov/39077777/
10. Gulati, M., Dursun, E., Vincent, K., & Watt, F. E. (2023). The influence of sex hormones on musculoskeletal pain and osteoarthritis. Lancet Rheumatology, 5(4), e225–e238. https://pubmed.ncbi.nlm.nih.gov/38251525/
11. Kling, J. M., MacLaughlin, K. L., Schnatz, P. F., et al. (2019). Menopause management knowledge in postgraduate family medicine, internal medicine, and obstetrics and gynecology residents: A cross-sectional survey. Mayo Clinic Proceedings, 94(2), 242–253. https://pubmed.ncbi.nlm.nih.gov/30711122/
12. Jeevananthan, A., Alexopoulos, A. S., Goldstein, K. M., & Moreno, A. C. (2025). Perceptions of menopause care: A pilot survey study of providers from primary care, endocrinology, and obstetrics and gynecology. Journal of Women's Health.https://pubmed.ncbi.nlm.nih.gov/40844489/
This content is for educational purposes only and is not a substitute for personalized medical advice. Consult your healthcare provider for guidance specific to your situation.